

HIGHLIGHTS
- Italy, Spain, Sweden have requested immediate withdrawal of several types of masks or have prohibited their use due to ineffectiveness
- A number of US States have lifted their mask mandates
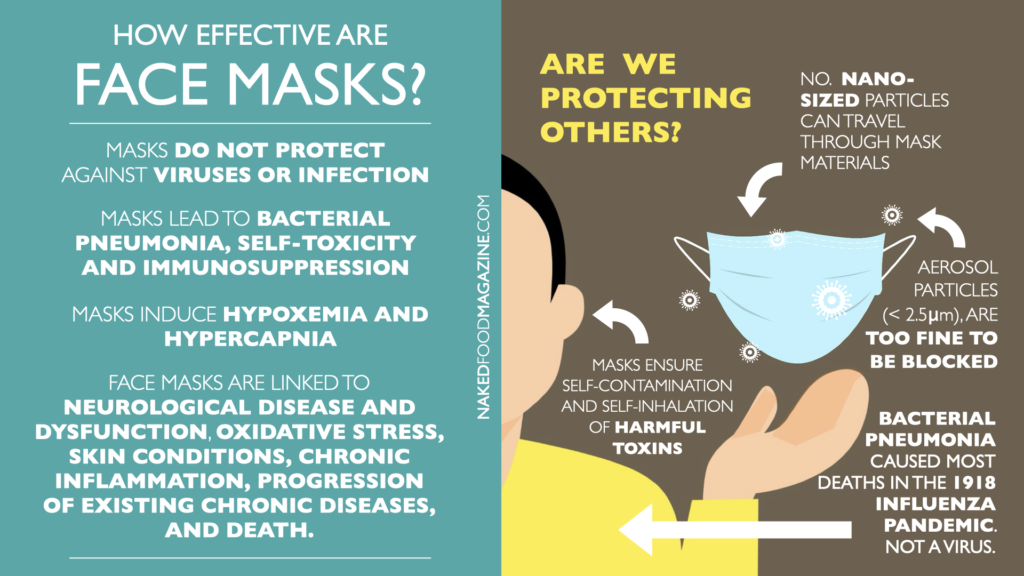
- Masks do not protect against viruses or other nano-sized particles
- Sars-Cov-2 has never been isolated or proven to be the cause of Covid19 disease
- Masks lead to Bacterial Pneumonia, self-toxicity and immunosuppression
- Masks induce hypoxemia and hypercapnia
- The use of face masks is linked to neurological disease and dysfunction, oxidative stress, skin conditions, chronic inflammation, progression of existing chronic diseases, and death.
The Office of the Attorney General in Gorizia, Italy, [1] has banned the use of face masks due to their lack of effectiveness, under the directive of the Italian law enforcement agency.[2]
Approximately 190 million masks in circulation, categorized as “better protection than others”, such as the KN95, FFP2, and FFP3, are now being recalled. The original document can be found here. According to an examination conducted by two Italian laboratories, one in Turin and another in Milan, half of the masks imported from China “do not protect enough from the risk of infection, as they do not filter sufficiently”.
Besides the masks in question, there have been other types of masks, such as those created by FCA (Fiat and Chrysler) in Italy, which have also been considered ineffective according to the standards.[3] These masks have been selected and provided as the official products by the government itself for school children, medical and health staff, and other public workers.
Officials in the municipality of Halmstad, Sweden, recently also prohibited the use of masks and all forms of PPE in schools. The municipality stated that, there was no scientific evidence for wearing masks, citing the Swedish public health agency.[4]
The Professional Union of the Ertzaintza (SiPE) in Spain, has requested the immediate withdrawal of all the FFP2 masks due to possible pulmonary risks in whose composition graphene is present, and which have been supplied in police centers.[5]
In the United States, the states and territories already without mask mandates include Alabama, Alaska, Arizona, Arkansas, Florida, Georgia, Idaho, Indiana, Iowa, Kansas, Mississippi, Missouri, Montana, Nebraska, North Dakota, Northern Mariana Islands, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, Wisconsin and Wyoming.[6]
Mask effectiveness is provided by the manufacturer on the product’s packaging. Boxes clearly state that these masks offer “some effectivity” in filtering certain particles.[7] In the case of the standard ear loop masks, the package claims “this product is an ear loop mask, not a respirator and will not provide any protection against COVID-19 (coronavirus) and other viruses or contaminants.” [8] This has been public knowledge since the beginning of the Covid-19 situation.
Face masks claim protection from particles as small as 1 micron, although viral particles including those of Sars-Cov-2 are nanoparticles and are measured in nanometers.[9] [10] 1 micron equals 1000 nanometers,[11] thus, the smallest area of fabric tissue in a face mask is 1000 times larger than any viral particle.[12]
Regardless of the mask quality, origin, or manufacturer, whether considered approved or non-approved by authorities, no mask available on the market can filter nanometer particles. Therefore, no mask can provide any protection or filtering of viral particles.
It is also vital to acknowledge that, no health institution, agency, university, academic institution, pharmaceutical company, research lab, government, other health entities or institutions, have been able to demonstrate or show proof of virus purification and isolation[13] for Sars-Cov-2 or any other viruses known to man. Virus purification and isolation is the fundamental scientific requirement, to prove the existence of a contagious agent or virus and/or its assumed infectivity.
Who gains? The global disposable face mask market size exceeded a value of USD 74.90 billion in only the first Quarter of 2020.[14] It is expected to grow 53.0% annually until 2027; however, absolutely no funds have been invested on informing people about the consequences of depriving the human body from inhaling oxygen—as humans depend on oxygen for respiration and life—as well as the devastating consequences of wearing masks [15] as explained below.
Breathing is an essential process for removing metabolic byproducts [carbon dioxide (CO2)] occurring during cell respiration.[16] [17] Trapped air remaining between the mouth, nose and the facemask is rebreathed repeatedly in and out of the body, containing low O2 and high CO2 concentrations, causing hypoxemia (below-normal level of oxygen in the blood) and hypercapnia (buildup of carbon dioxide in the bloodstream).[18] [19] [20] [21] [22]
Chronic mild or moderate hypoxemia and hypercapnia such as from wearing facemasks is linked to higher anaerobic energy metabolism, decrease in pH levels and increase in cells and blood acidity, toxicity, neurological disease and dysfunction, [23][24] oxidative stress, skin conditions, chronic inflammation, immunosuppression,[25] [26] [27] [28] health deterioration, and death.[29][30] [31] [32] [33]
Severe hypoxemia may also provoke cardiopulmonary and neurological complications and is considered an important clinical sign in cardiopulmonary medicine.[34] [35] [36] [37] [38] [39] Low oxygen content in the arterial blood can cause myocardial ischemia, serious arrhythmias, right or left ventricular dysfunction, dizziness, hypotension, syncope and pulmonary hypertension.[40]
The graphic below summarizes the physiological and psychological effects of wearing face masks and their potential long-term consequences for health.[41]
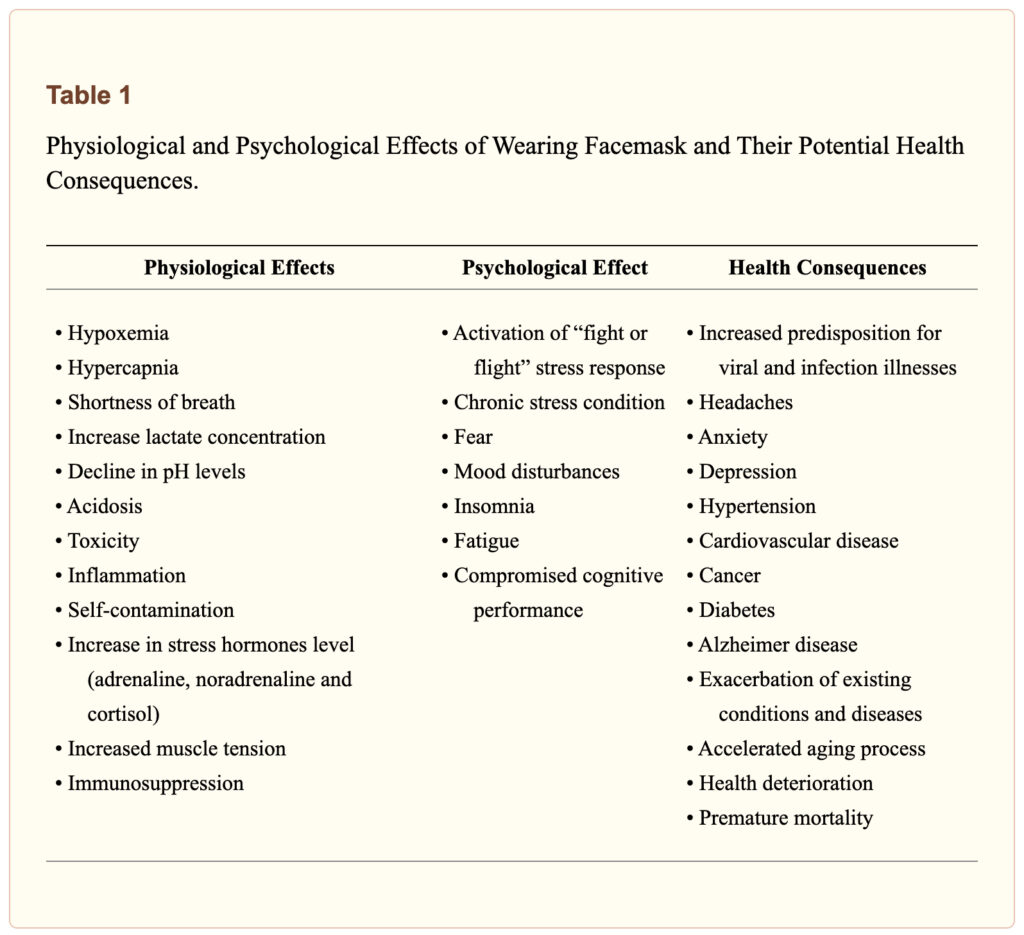
Even though the long-term wearing of face masks has devastating health consequences, governmental institutions and health agencies continue forcing people to wear masks from the beginning of 2020. Prolonged hypoxic-hypercapnic state compromises the normal physiological and psychological balance, deteriorates health, and promotes the developing and progression of existing chronic diseases.[42] [43] [44] [45] [46] [47] [48]
In addition to hypoxia and hypercapnia, individuals are inhaling residues of bacterial and pathogen components on the inner and outside layer of the face mask. These toxic components are repeatedly rebreathed back into the body, causing self-contamination.[49]
Breathing through face masks also increases temperature and humidity in the space between the mouth and the mask, resulting in a release of toxic particles from the mask’s materials.[50] [51] [52] [53] [54] [55]
Rebreathing contaminated air with high bacterial and toxic particle concentrations along with low O2 and high CO2 levels continuously challenge the body’s homeostasis, causing self-toxicity and immunosuppression.[56] [57] [58] [59] [60] [61]
According to a 2015 scientific paper written by Anthony Fauci himself,[62] and published by the National Institute of Health, Bacterial Pneumonia caused most deaths in the 1918 influenza pandemic, and not a virus.[63] The pneumonia was caused when bacteria that normally inhabit the nose and throat entered the lungs.
In conclusion, the use of face masks is not only unnecessary, ineffective, and dangerous, but it is also extremely harmful for Physiological and Psychological health. Many countries, cities, and tribunals are declaring the use of facemasks unconstitutional and a threat to public health while the mainstream narrative continues to promote it. Those who insist in instituting and encouraging these unscientific and dangerous public policies should be legally prosecuted for crimes against humanity.
Photo Credit:
Image by leo2014 from Pixabay
___
References
[1] Renzo. “In Italy There Are 190 Million. Lots at Risk.” Italy24 News English, Italy24 News English, 13 Apr. 2021, www.italy24news.com/News/17630.html.
[2] Procura Di Gorizia.
[3] Raia, di Davide. “FCA Italy Denunciata: Le Sue Mascherine Non Sarebbero a Norma.” ClubAlfa.it, 26 Jan. 2021, www.clubalfa.it/325909-fca-italy-denunciata-le-sue-mascherine-non-sarebbero-a-norma.
[4] Sveriges Radio. “Halmstad Förbjuder Munskydd i Skolan – P4 Halland.” P4 Halland | Sveriges Radio, Sveriges Radio, 23 Jan. 2021, sverigesradio.se/artikel/halmstad-forbjuder-munskydd-i-skolan.
[5] EITB Euskal Irrati Telebista. “SiPE Pide La Retirada De Las Mascarillas FFP2 Con Grafeno Entregadas a La Ertzaintza.” EITB Radio Televisión Pública Vasca, EITB Euskal Irrati Telebista, 14 Apr. 2021, www.eitb.eus/es/noticias/sociedad/detalle/7978384/sipe-pide-retirada-mascarillas-ffp2-grafeno/?utm_source=break.ma&utm_medium=break.ma.
[6] “These States Have COVID-19 Mask Mandates.” U.S. News & World Report, U.S. News & World Report, www.usnews.com/news/best-states/articles/these-are-the-states-with-mask-mandates.
[7] Particulate Respirator N95.
[8] “It’s On The Box: Face Masks Mandated By UK Government Don’t Protect Against COVID-19.” The World We Live In, 17 July 2020, luis46pr.wordpress.com/2020/07/17/its-on-the-box-face-masks-mandated-by-uk-government-dont-protect-against-covid-19/.
[9] Wiersinga W.J., Rhodes A., Cheng A.C., Peacock S.J., Prescott H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA. 2020
[10] Zhu N., Zhang D., Wang W., Li X., Yang B., Song J. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020;382:727–733.
[11] “Nanoparticle Size.” Nanoparticle Size – an Overview | ScienceDirect Topics, www.sciencedirect.com/topics/chemistry/nanoparticle-size.
[12] Konda A., Prakash A., Moss G.A., Schmoldt M., Grant G.D., Guha S. Aerosol Filtration Efficiency of Common Fabrics Used in Respiratory Cloth Masks. ACS Nano. 2020;14:6339–6347.
[13] “FOIs Reveal That Health/Science Institutions around the World Have No Record of SARS-COV-2 Isolation/Purification, Anywhere, Ever.” Fluoride Free Peel, www.fluoridefreepeel.ca/fois-reveal-that-health-science-institutions-around-the-world-have-no-record-of-sars-cov-2-isolation-purification/.
[14] Disposable Face Mask Market Size Report, 2020-2027, www.grandviewresearch.com/industry-analysis/disposable-face-masks-market.
[15] Vainshelboim, Baruch. “Facemasks in the COVID-19 Era: A Health Hypothesis.” Medical Hypotheses, Elsevier Ltd., Jan. 2021, www.ncbi.nlm.nih.gov/pmc/articles/PMC7680614/.
[16] Farrell P.A., Joyner M.J., Caiozzo V.J. second edition. Lippncott Williams & Wilkins; Baltimore: 2012. ACSM’s Advanced Exercise Physiology.
[17] Kenney W.L., Wilmore J.H., Costill D.L. 5th ed. Human Kinetics; Champaign, IL: 2012. Physiology of sport and exercise.
[18] Kao T.W., Huang K.C., Huang Y.L., Tsai T.J., Hsieh B.S., Wu M.S. The physiological impact of wearing an N95 mask during hemodialysis as a precaution against SARS in patients with end-stage renal disease. J Formos Med Assoc. 2004;103:624–628.
[19] United States Department of Labor. Occupational Safety and Health Administration. Respiratory Protection Standard, 29 CFR 1910.134; 2007.
[20] American College of Sports Medicine . Sixth ed. Lippincott Wiliams & Wilkins; Baltimore: 2010. ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription.
[21] Farrell P.A., Joyner M.J., Caiozzo V.J. second edition. Lippncott Williams & Wilkins; Baltimore: 2012. ACSM’s Advanced Exercise Physiology.
[22] Kenney W.L., Wilmore J.H., Costill D.L. 5th ed. Human Kinetics; Champaign, IL: 2012. Physiology of sport and exercise.[23] RT;, Ryou MG;Mallet. “An In Vitro Oxygen-Glucose Deprivation Model for Studying Ischemia-Reperfusion Injury of Neuronal Cells.” Methods in Molecular Biology (Clifton, N.J.), U.S. National Library of Medicine, pubmed.ncbi.nlm.nih.gov/29468596/.
[24] B;, Tornabene E;Helms HCC;Pedersen SF;Brodin. “Effects of Oxygen-Glucose Deprivation (OGD) on Barrier Properties and MRNA Transcript Levels of Selected Marker Proteins in Brain Endothelial Cells/Astrocyte Co-Cultures.” PloS One, U.S. National Library of Medicine, pubmed.ncbi.nlm.nih.gov/31425564/.
[25] A;, Ohta. “Oxygen-Dependent Regulation of Immune Checkpoint Mechanisms.” International Immunology, U.S. National Library of Medicine, pubmed.ncbi.nlm.nih.gov/29846615/.
[26] RS;, Palazon A;Goldrath AW;Nizet V;Johnson. “HIF Transcription Factors, Inflammation, and Immunity.” Immunity, U.S. National Library of Medicine, pubmed.ncbi.nlm.nih.gov/25367569/.
[27] EL;, Colgan SP;Campbell. “Oxygen Metabolism and Innate Immune Responses in the Gut.” Journal of Applied Physiology (Bethesda, Md. : 1985), U.S. National Library of Medicine, pubmed.ncbi.nlm.nih.gov/28705991/.
[28] Zhang X;Fu C;Chen B;Xu Z;Zeng Z;He L;Lu Y;Chen Z;Liu X; “Autophagy Induced by Oxygen-Glucose Deprivation Mediates the Injury to the Neurovascular Unit.” Medical Science Monitor : International Medical Journal of Experimental and Clinical Research, U.S. National Library of Medicine, pubmed.ncbi.nlm.nih.gov/30787267/.
[29] Chandrasekaran B., Fernandes S. “Exercise with facemask; Are we handling a devil’s sword?” – A physiological hypothesis. Med Hypotheses. 2020;144
[30] American College of Sports Medicine . Sixth ed. Lippincott Wiliams & Wilkins; Baltimore: 2010. ACSM’s Resource Manual for Guidelines for Exercise Testing and Priscription.
[31] Farrell P.A., Joyner M.J., Caiozzo V.J. second edition. Lippncott Williams & Wilkins; Baltimore: 2012. ACSM’s Advanced Exercise Physiology.[32] Kenney W.L., Wilmore J.H., Costill D.L. 5th ed. Human Kinetics; Champaign, IL: 2012. Physiology of sport and exercise.
[33] PR;, Granger DN;Kvietys. “Reperfusion Injury and Reactive Oxygen Species: The Evolution of a Concept.” Redox Biology, U.S. National Library of Medicine, pubmed.ncbi.nlm.nih.gov/26484802/.
[34] ATS/ACCP Statement on cardiopulmonary exercise testing Am J Respir Crit Care Med. 2003;167:211–277.
[35] American College of Sports Medicine . 9th ed. Wolters Kluwer/Lippincott Williams & Wilkins Health; Philadelphia: 2014. ACSM’s guidelines for exercise testing and prescription.
[36] Balady G.J., Arena R., Sietsema K., Myers J., Coke L., Fletcher G.F. Clinician’s Guide to cardiopulmonary exercise testing in adults: a scientific statement from the American Heart Association. Circulation. 2010;122:191–225. [37] Ferrazza A.M., Martolini D., Valli G., Palange P. Cardiopulmonary exercise testing in the functional and prognostic evaluation of patients with pulmonary diseases. Respiration. 2009;77:3–17. [38] Fletcher G.F., Ades P.A., Kligfield P., Arena R., Balady G.J., Bittner V.A. Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation. 2013;128:873–934. [39] Guazzi M., Adams V., Conraads V., Halle M., Mezzani A., Vanhees L. EACPR/AHA Scientific Statement. Clinical recommendations for cardiopulmonary exercise testing data assessment in specific patient populations. Circulation. 2012;126:2261–2274.[40] Naeije R., Dedobbeleer C. Pulmonary hypertension and the right ventricle in hypoxia. Exp Physiol. 2013;98:1247–1256.
[41] Vainshelboim, Baruch. “Facemasks in the COVID-19 Era: A Health Hypothesis.” Medical Hypotheses, Elsevier Ltd., Jan. 2021, www.ncbi.nlm.nih.gov/pmc/articles/PMC7680614/.
[42] Lurie K.G., Nemergut E.C., Yannopoulos D., Sweeney M. The Physiology of Cardiopulmonary Resuscitation. Anesth Analg. 2016;122:767–783.
[43] American College of Sports Medicine . 9th ed. Wolters Kluwer/Lippincott Williams & Wilkins Health; Philadelphia: 2014. ACSM’s guidelines for exercise testing and prescription.[44] Balady G.J., Arena R., Sietsema K., Myers J., Coke L., Fletcher G.F. Clinician’s Guide to cardiopulmonary exercise testing in adults: a scientific statement from the American Heart Association. Circulation. 2010;122:191–225.
[45] Naeije R., Dedobbeleer C. Pulmonary hypertension and the right ventricle in hypoxia. Exp Physiol. 2013;98:1247–1256.
[46] Schneiderman N., Ironson G., Siegel S.D. Stress and health: psychological, behavioral, and biological determinants. Annu Rev Clin Psychol. 2005;1:607–628.
[47] Thoits P.A. Stress and health: major findings and policy implications. J Health Soc Behav. 2010;51(Suppl):S41–S53.
[48] World Health Organization. World health statistics 2018: monitoring health for the SDGs, sustainable development goals Geneva, Switzerland; 2018.
[49] Vainshelboim, Baruch. “Facemasks in the COVID-19 Era: A Health Hypothesis.” Medical Hypotheses, Elsevier Ltd., Jan. 2021, www.ncbi.nlm.nih.gov/pmc/articles/PMC7680614/.
[50] Fisher E.M., Noti J.D., Lindsley W.G., Blachere F.M., Shaffer R.E. Validation and application of models to predict facemask influenza contamination in healthcare settings. Risk Anal. 2014;34:1423–1434.
[51] World Health Organization. Advice on the use of masks in the context of COVID-19. Geneva, Switzerland; 2020.
[52] MacIntyre C.R., Seale H., Dung T.C., Hien N.T., Nga P.T., Chughtai A.A. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ open. 2015;5
[53] Leung N.H.L., Chu D.K.W., Shiu E.Y.C., Chan K.H., McDevitt J.J., Hau B.J.P. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat Med. 2020;26:676–680.
[54] Kao T.W., Huang K.C., Huang Y.L., Tsai T.J., Hsieh B.S., Wu M.S. The physiological impact of wearing an N95 mask during hemodialysis as a precaution against SARS in patients with end-stage renal disease. J Formos Med Assoc. 2004;103:624–628.
[55] United States Department of Labor. Occupational Safety and Health Administration. Respiratory Protection Standard, 29 CFR 1910.134; 2007.[56] Fisher E.M., Noti J.D., Lindsley W.G., Blachere F.M., Shaffer R.E. Validation and application of models to predict facemask influenza contamination in healthcare settings. Risk Anal. 2014;34:1423–1434.
[57] World Health Organization. Advice on the use of masks in the context of COVID-19. Geneva, Switzerland; 2020.
[58] MacIntyre C.R., Seale H., Dung T.C., Hien N.T., Nga P.T., Chughtai A.A. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ open. 2015;5
[59] Leung N.H.L., Chu D.K.W., Shiu E.Y.C., Chan K.H., McDevitt J.J., Hau B.J.P. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat Med. 2020;26:676–680.
[60] Kao T.W., Huang K.C., Huang Y.L., Tsai T.J., Hsieh B.S., Wu M.S. The physiological impact of wearing an N95 mask during hemodialysis as a precaution against SARS in patients with end-stage renal disease. J Formos Med Assoc. 2004;103:624–628.
[61] United States Department of Labor. Occupational Safety and Health Administration. Respiratory Protection Standard, 29 CFR 1910.134; 2007.[62] AS;, Morens DM;Taubenberger JK;Fauci. “Predominant Role of Bacterial Pneumonia as a Cause of Death in Pandemic Influenza: Implications for Pandemic Influenza Preparedness.” The Journal of Infectious Diseases, U.S. National Library of Medicine, pubmed.ncbi.nlm.nih.gov/18710327/.
[63] “Bacterial Pneumonia Caused Most Deaths in 1918 Influenza Pandemic.” National Institutes of Health, U.S. Department of Health and Human Services, 23 Sept. 2015, www.nih.gov/news-events/news-releases/bacterial-pneumonia-caused-most-deaths-1918-influenza-pandemic.
Tags
neurological disease nanoparticles immunosuppression carbon dioxide KN95 death oxygen FFP2 FFP3 ineffectiveness pulmonary Italy hypoxemia hypercapnia mask blood acidity covid toxicity sars-cov-2The Author
You Might Also Like




















{kind=link}
November 8, 2023
This article is misleading. The fact that even one of the references was misspelled casts doubt.
November 22, 2023
It is not. None of the references are misspelled and the sources are accurate.
February 21, 2022
This is the first site with an article that uses references and sources. There are a lot for this particular topic.
March 24, 2022
Yes, thank you :) There are many more references and sources since this article was posted. We will try to update it soon as well!
December 3, 2021
stick with food and not bashing science
February 4, 2022
Science is the observation, identification, description, experimental investigation, and theoretical explanation of phenomena in the physical world. Science aims to explain NATURE through observation. We are pro-science and pro-evidence.
October 31, 2021
When I read a news how I can know the date you post it? I cannot find it.
March 24, 2022
Hello, thank you for commenting. We will add dates to the posts.
April 22, 2021
“Officials in the municipality of Halmstad, Sweden, recently also prohibited the use of masks and all forms of PPE in schools. The municipality stated that, there was no scientific evidence for wearing masks, citing the Swedish public health agency.[4]”
Teachers Union wanted to keep this recommendation, so the municipality of Halmstad had to surrender. Otherwise, Schweden don`t have a recommendation for using masks
April 19, 2021
The ban is on homemade cloth facemasks. This article is horribly misleading.
April 21, 2021
That’s not correct, and your comment is very misleading. In terms of Spain and Sweden, please follow the respective references. In terms of Italy, the ban is not for “homemade cloth masks” as you state. The recall refers to manufactured masks that include KN95, FFP2, and FFP3. The decret can be downloaded here: https://nakedfoodmagazine.com/4_6026179028589742176.pdf